Does time spent using digital technology and social media have an adverse effect on mental health, especially that of adolescents? Here, two scientists discuss the question, and how digital devices might be used to improve well-being.
• There is an ongoing debate about whether social media and the use of digital devices are detrimental to mental health.
• Adolescents tend to be heavy users of these devices, and especially of social media.
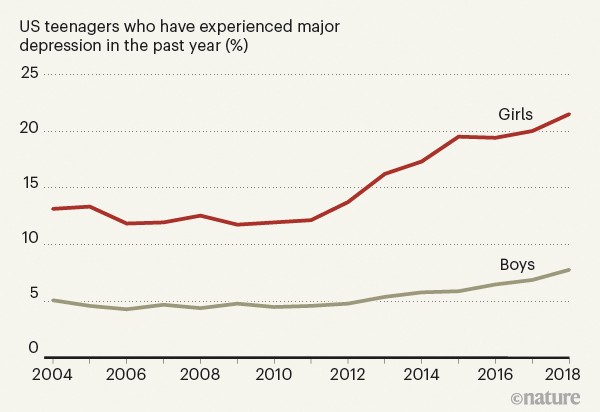
• Rates of teenage depression began to rise around 2012, when adolescent use of social media became common (Fig. 1).
• Some evidence indicates that frequent users of social media have higher rates of depression and anxiety than do light users.
• But perhaps digital devices could provide a way of gathering data about mental health in a systematic way, and make interventions more timely.
A sudden increase in the rates of depression, anxiety and self-harm was seen in adolescents — particularly girls — in the United States and the United Kingdom around 2012 or 2013 (see go.nature.com/2up38hw). Only one suspect was in the right place at the right time to account for this sudden change: social media. Its use by teenagers increased most quickly between 2009 and 2011, by which point two-thirds of 15–17-year-olds were using it on a daily basis 1 . Some researchers defend social media, arguing that there is only circumstantial evidence for its role in mental-health problems 2 , 3 . And, indeed, several studies 2 , 3 show that there is only a small correlation between time spent on screens and bad mental-health outcomes. However, I present three arguments against this defence.
First, the papers that report small or null effects usually focus on ‘screen time’, but it is not films or video chats with friends that damage mental health. When research papers allow us to zoom in on social media, rather than looking at screen time as a whole, the correlations with depression are larger, and they are larger still when we look specifically at girls (go.nature.com/2u74der). The sex difference is robust, and there are several likely causes for it. Girls use social media much more than do boys (who, in turn, spend more of their time gaming). And, for girls more than boys, social life and status tend to revolve around intimacy and inclusion versus exclusion 4 , making them more vulnerable to both the ‘fear of missing out’ and the relational aggression that social media facilitates.
Second, although correlational studies can provide only circumstantial evidence, most of the experiments published in recent years have found evidence of causation (go.nature.com/2u74der). In these studies, people are randomly assigned to groups that are asked to continue using social media or to reduce their use substantially. After a few weeks, people who reduce their use generally report an improvement in mood or a reduction in loneliness or symptoms of depression.
The best way forward
Third, many researchers seem to be thinking about social media as if it were sugar: safe in small to moderate quantities, and harmful only if teenagers consume large quantities. But, unlike sugar, social media does not act just on those who consume it. It has radically transformed the nature of peer relationships, family relationships and daily activities 5 . When most of the 11-year-olds in a class are on Instagram (as was the case in my son’s school), there can be pervasive effects on everyone. Children who opt out can find themselves isolated. A simple dose–response model cannot capture the full effects of social media, yet nearly all of the debate among researchers so far has been over the size of the dose–response effect. To cite just one suggestive finding of what lies beyond that model: network effects for depression and anxiety are large, and bad mental health spreads more contagiously between women than between men 6 .
In conclusion, digital media in general undoubtedly has many beneficial uses, including the treatment of mental illness. But if you focus on social media, you’ll find stronger evidence of harm, and less exculpatory evidence, especially for its millions of under-age users.
What should we do while researchers hash out the meaning of these conflicting findings? I would urge a focus on middle schools (roughly 11–13-year-olds in the United States), both for researchers and policymakers. Any US state could quickly conduct an informative experiment beginning this September: randomly assign a portion of school districts to ban smartphone access for students in middle school, while strongly encouraging parents to prevent their children from opening social-media accounts until they begin high school (at around 14). Within 2 years, we would know whether the policy reversed the otherwise steady rise of mental-health problems among middle-school students, and whether it also improved classroom dynamics (as rated by teachers) and test scores. Such system-wide and cross-school interventions would be an excellent way to study the emergent effects of social media on the social lives and mental health of today’s adolescents.
It is appealing to condemn social media out of hand on the basis of the — generally rather poor-quality and inconsistent — evidence suggesting that its use is associated with mental-health problems 7 . But focusing only on its potential harmful effects is comparable to proposing that the only question to ask about cars is whether people can die driving them. The harmful effects might be real, but they don’t tell the full story. The task of research should be to understand what patterns of digital-device and social-media use can lead to beneficial versus harmful effects 7 , and to inform evidence-based approaches to policy, education and regulation.
Long-standing problems have hampered our efforts to improve access to, and the quality of, mental-health services and support. Digital technology has the potential to address some of these challenges. For instance, consider the challenges associated with collecting data on human behaviour. Assessment in mental-health care and research relies almost exclusively on self-reporting, but the resulting data are subjective and burdensome to collect. As a result, assessments are conducted so infrequently that they do not provide insights into the temporal dynamics of symptoms, which can be crucial for both diagnosis and treatment planning.
By contrast, mobile phones and other Internet-connected devices provide an opportunity to continuously collect objective information on behaviour in the context of people’s real lives, generating a rich data set that can provide insight into the extent and timing of mental-health needs in individuals 8 , 9 . By building apps that can track our digital exhaust (the data generated by our everyday digital lives, including our social-media use), we can gain insights into aspects of behaviour that are well-established building blocks of mental health and illness, such as mood, social communication, sleep and physical activity.

Stress and the city
These data can, in turn, be used to empower individuals, by giving them actionable insights into patterns of behaviour that might otherwise have remained unseen. For example, subtle shifts in patterns of sleep or social communication can provide early warning signs of deteriorating mental health. Data on these patterns can be used to alert people to the need for self-management before the patterns — and the associated symptoms — become more severe. Individuals can also choose to share these data with health professionals or researchers. For instance, in the Our Data Helps initiative, individuals who have experienced a suicidal crisis, or the relatives of those who have died by suicide, can donate their digital data to research into suicide risk.
Because mobile devices are ever-present in people’s lives, they offer an opportunity to provide interventions that are timely, personalized and scalable. Currently, mental-health services are mainly provided through a century-old model in which they are made available at times chosen by the mental-health practitioner, rather than at the person’s time of greatest need. But Internet-connected devices are facilitating the development of a wave of ‘just-in-time’ interventions 10 for mental-health care and support.
A compelling example of these interventions involves short-term risk for suicide 9 , 11 — for which early detection could save many lives. Most of the effective approaches to suicide prevention work by interrupting suicidal actions and supporting alternative methods of coping at the moment of greatest risk. If these moments can be detected in an individual’s digital exhaust, a wide range of intervention options become available, from providing information about coping skills and social support, to the initiation of crisis responses. So far, just-in-time approaches have been applied mainly to behaviours such as eating or substance abuse 8 . But with the development of an appropriate research base, these approaches have the potential to provide a major advance in our ability to respond to, and prevent, mental-health crises.
These advantages are particularly relevant to teenagers. Because of their extensive use of digital devices, adolescents are especially vulnerable to the devices’ risks and burdens. And, given the increases in mental-health problems in this age group, teens would also benefit most from improvements in mental-health prevention and treatment. If we use the social and data-gathering functions of Internet-connected devices in the right ways, we might achieve breakthroughs in our ability to improve mental health and well-being.
Nature 578, 226-227 (2020)